HAEM5:Myelodysplastic neoplasm with low blasts and 5q deletion: Difference between revisions
Bailey.Glen (talk | contribs) No edit summary |
Bailey.Glen (talk | contribs) No edit summary |
||
| Line 72: | Line 72: | ||
<blockquote class='blockedit'>{{Box-round|title=v4:Clinical Features|The content below was from the old template. Please incorporate above.}} | <blockquote class='blockedit'>{{Box-round|title=v4:Clinical Features|The content below was from the old template. Please incorporate above.}}</blockquote> | ||
*Macrocytic anemia most common, usually severe and can be transfusion dependent. | *Macrocytic anemia most common, usually severe and can be transfusion dependent. | ||
| Line 79: | Line 79: | ||
*Good prognosis and low risk to progress to AML. | *Good prognosis and low risk to progress to AML. | ||
<blockquote class="blockedit"> | |||
<center><span style="color:Maroon">'''End of V4 Section'''</span> | |||
---- | |||
</blockquote> | </blockquote> | ||
==Sites of Involvement== | ==Sites of Involvement== | ||
| Line 107: | Line 110: | ||
<blockquote class='blockedit'>{{Box-round|title=v4:Immunophenotype|The content below was from the old template. Please incorporate above.}} | <blockquote class='blockedit'>{{Box-round|title=v4:Immunophenotype|The content below was from the old template. Please incorporate above.}}</blockquote> | ||
There is no distinct immunophenotypic profile specific for myelodysplastic syndrome (MDS) with isolated del(5q). Currently, morphologic evaluation remains the gold standard in diagnosis of MDS. Immunophenotyping provides supportive evidence to clarify the blasts nature and percentage <ref>{{Cite journal|last=Zini|first=Gina|date=2017|title=Diagnostics and Prognostication of Myelodysplastic Syndromes|url=https://synapse.koreamed.org/DOIx.php?id=10.3343/alm.2017.37.6.465|journal=Annals of Laboratory Medicine|language=en|volume=37|issue=6|pages=465|doi=10.3343/alm.2017.37.6.465|issn=2234-3806|pmc=PMC5587818|pmid=28840983}}</ref>. | There is no distinct immunophenotypic profile specific for myelodysplastic syndrome (MDS) with isolated del(5q). Currently, morphologic evaluation remains the gold standard in diagnosis of MDS. Immunophenotyping provides supportive evidence to clarify the blasts nature and percentage <ref>{{Cite journal|last=Zini|first=Gina|date=2017|title=Diagnostics and Prognostication of Myelodysplastic Syndromes|url=https://synapse.koreamed.org/DOIx.php?id=10.3343/alm.2017.37.6.465|journal=Annals of Laboratory Medicine|language=en|volume=37|issue=6|pages=465|doi=10.3343/alm.2017.37.6.465|issn=2234-3806|pmc=PMC5587818|pmid=28840983}}</ref>. | ||
<blockquote class="blockedit"> | |||
<center><span style="color:Maroon">'''End of V4 Section'''</span> | |||
---- | |||
</blockquote> | </blockquote> | ||
==Chromosomal Rearrangements (Gene Fusions)== | ==Chromosomal Rearrangements (Gene Fusions)== | ||
| Line 135: | Line 141: | ||
<blockquote class='blockedit'>{{Box-round|title=v4:Chromosomal Rearrangements (Gene Fusions)|The content below was from the old template. Please incorporate above.}} | <blockquote class='blockedit'>{{Box-round|title=v4:Chromosomal Rearrangements (Gene Fusions)|The content below was from the old template. Please incorporate above.}}</blockquote> | ||
NA | NA | ||
| Line 148: | Line 154: | ||
|} | |} | ||
<blockquote class="blockedit"> | |||
<center><span style="color:Maroon">'''End of V4 Section'''</span> | |||
---- | |||
</blockquote> | </blockquote> | ||
| Line 155: | Line 164: | ||
* Individual Region Genomic Gain/Loss/LOH | * Individual Region Genomic Gain/Loss/LOH | ||
* Characteristic Chromosomal Patterns | * Characteristic Chromosomal Patterns | ||
* Gene Mutations (SNV/INDEL)}} | * Gene Mutations (SNV/INDEL)}}</blockquote> | ||
<u>Diagnosis:</u> | <u>Diagnosis:</u> | ||
| Line 175: | Line 184: | ||
Lenalidomide is an analogue of thalidomide which functions as an immunomodulatory agent. Treatment with lenalidomide has shown great potential in reducing the abnormal clone as well as transfusion dependency irrespective of cytogenetic complexity <ref>{{Cite journal|last=Giagounidis|first=A. A. N.|last2=Germing|first2=U.|last3=Strupp|first3=C.|last4=Hildebrandt|first4=B.|last5=Heinsch|first5=M.|last6=Aul|first6=C.|date=2005|title=Prognosis of patients with del(5q) MDS and complex karyotype and the possible role of lenalidomide in this patient subgroup|url=http://link.springer.com/10.1007/s00277-005-1054-0|journal=Annals of Hematology|language=en|volume=84|issue=9|pages=569–571|doi=10.1007/s00277-005-1054-0|issn=0939-5555}}</ref><ref>{{Cite journal|last=List|first=Alan|last2=Dewald|first2=Gordon|last3=Bennett|first3=John|last4=Giagounidis|first4=Aristotle|last5=Raza|first5=Azra|last6=Feldman|first6=Eric|last7=Powell|first7=Bayard|last8=Greenberg|first8=Peter|last9=Thomas|first9=Deborah|date=2006|title=Lenalidomide in the Myelodysplastic Syndrome with Chromosome 5q Deletion|url=http://www.nejm.org/doi/abs/10.1056/NEJMoa061292|journal=New England Journal of Medicine|language=en|volume=355|issue=14|pages=1456–1465|doi=10.1056/NEJMoa061292|issn=0028-4793}}</ref>. FDA approved [https://www.accessdata.fda.gov/drugsatfda_docs/label/2012/021880s028lbl.pdf Lenalidomide] on December 2005 for treating MDS with del(5q) with or without additional cytogenetic abnormalities. | Lenalidomide is an analogue of thalidomide which functions as an immunomodulatory agent. Treatment with lenalidomide has shown great potential in reducing the abnormal clone as well as transfusion dependency irrespective of cytogenetic complexity <ref>{{Cite journal|last=Giagounidis|first=A. A. N.|last2=Germing|first2=U.|last3=Strupp|first3=C.|last4=Hildebrandt|first4=B.|last5=Heinsch|first5=M.|last6=Aul|first6=C.|date=2005|title=Prognosis of patients with del(5q) MDS and complex karyotype and the possible role of lenalidomide in this patient subgroup|url=http://link.springer.com/10.1007/s00277-005-1054-0|journal=Annals of Hematology|language=en|volume=84|issue=9|pages=569–571|doi=10.1007/s00277-005-1054-0|issn=0939-5555}}</ref><ref>{{Cite journal|last=List|first=Alan|last2=Dewald|first2=Gordon|last3=Bennett|first3=John|last4=Giagounidis|first4=Aristotle|last5=Raza|first5=Azra|last6=Feldman|first6=Eric|last7=Powell|first7=Bayard|last8=Greenberg|first8=Peter|last9=Thomas|first9=Deborah|date=2006|title=Lenalidomide in the Myelodysplastic Syndrome with Chromosome 5q Deletion|url=http://www.nejm.org/doi/abs/10.1056/NEJMoa061292|journal=New England Journal of Medicine|language=en|volume=355|issue=14|pages=1456–1465|doi=10.1056/NEJMoa061292|issn=0028-4793}}</ref>. FDA approved [https://www.accessdata.fda.gov/drugsatfda_docs/label/2012/021880s028lbl.pdf Lenalidomide] on December 2005 for treating MDS with del(5q) with or without additional cytogenetic abnormalities. | ||
<blockquote class="blockedit"> | |||
<center><span style="color:Maroon">'''End of V4 Section'''</span> | |||
---- | |||
</blockquote> | </blockquote> | ||
==Individual Region Genomic Gain / Loss / LOH== | ==Individual Region Genomic Gain / Loss / LOH== | ||
| Line 223: | Line 235: | ||
|} | |} | ||
<blockquote class='blockedit'>{{Box-round|title=v4:Genomic Gain/Loss/LOH|The content below was from the old template. Please incorporate above.}} | <blockquote class='blockedit'>{{Box-round|title=v4:Genomic Gain/Loss/LOH|The content below was from the old template. Please incorporate above.}}</blockquote> | ||
{| class="wikitable sortable" | {| class="wikitable sortable" | ||
| Line 234: | Line 246: | ||
|} | |} | ||
<blockquote class="blockedit"> | |||
<center><span style="color:Maroon">'''End of V4 Section'''</span> | |||
---- | |||
</blockquote> | </blockquote> | ||
==Characteristic Chromosomal Patterns== | ==Characteristic Chromosomal Patterns== | ||
| Line 258: | Line 273: | ||
|} | |} | ||
<blockquote class='blockedit'>{{Box-round|title=v4:Characteristic Chromosomal Aberrations / Patterns|The content below was from the old template. Please incorporate above.}} | <blockquote class='blockedit'>{{Box-round|title=v4:Characteristic Chromosomal Aberrations / Patterns|The content below was from the old template. Please incorporate above.}}</blockquote> | ||
The most characteristic cytogenetic abnormality is an interstitial deletion on the long arm of chromosome 5 or del(5q)<ref name=":0">{{Cite journal|last=Van Den Berghe|first=Herman|last2=Cassiman|first2=Jean-Jacques|last3=David|first3=Guido|last4=Fryns|first4=Jean-Pierre|last5=Michaux|first5=Jean-Louis|last6=Sokal|first6=Gerard|date=1974|title=Distinct haematological disorder with deletion of long arm of No. 5 chromosome|url=http://www.nature.com/articles/251437a0|journal=Nature|language=en|volume=251|issue=5474|pages=437–438|doi=10.1038/251437a0|issn=0028-0836}}</ref> The break point is not fixed but the region between bands q31 and q33 is generally deleted. Several candidates genes were thought to contribute to the haploinsufficiency effect of the deleted region, including ''RPS14'' <ref>{{Cite journal|last=Ebert|first=Benjamin L.|last2=Pretz|first2=Jennifer|last3=Bosco|first3=Jocelyn|last4=Chang|first4=Cindy Y.|last5=Tamayo|first5=Pablo|last6=Galili|first6=Naomi|last7=Raza|first7=Azra|last8=Root|first8=David E.|last9=Attar|first9=Eyal|date=2008|title=Identification of RPS14 as a 5q- syndrome gene by RNA interference screen|url=http://www.nature.com/articles/nature06494|journal=Nature|language=en|volume=451|issue=7176|pages=335–339|doi=10.1038/nature06494|issn=0028-0836|pmc=PMC3771855|pmid=18202658}}</ref>'', CSNK1A1'' <ref name=":1">{{Cite journal|last=Schneider|first=Rebekka K.|last2=Ademà|first2=Vera|last3=Heckl|first3=Dirk|last4=Järås|first4=Marcus|last5=Mallo|first5=Mar|last6=Lord|first6=Allegra M.|last7=Chu|first7=Lisa P.|last8=McConkey|first8=Marie E.|last9=Kramann|first9=Rafael|date=2014|title=Role of Casein Kinase 1A1 in the Biology and Targeted Therapy of del(5q) MDS|url=https://linkinghub.elsevier.com/retrieve/pii/S1535610814003353|journal=Cancer Cell|language=en|volume=26|issue=4|pages=509–520|doi=10.1016/j.ccr.2014.08.001|pmc=PMC4199102|pmid=25242043}}</ref>'','' miR-145 and miR-146a <ref>{{Cite journal|last=Starczynowski|first=Daniel T|last2=Kuchenbauer|first2=Florian|last3=Argiropoulos|first3=Bob|last4=Sung|first4=Sandy|last5=Morin|first5=Ryan|last6=Muranyi|first6=Andrew|last7=Hirst|first7=Martin|last8=Hogge|first8=Donna|last9=Marra|first9=Marco|date=2010|title=Identification of miR-145 and miR-146a as mediators of the 5q– syndrome phenotype|url=http://www.nature.com/articles/nm.2054|journal=Nature Medicine|language=en|volume=16|issue=1|pages=49–58|doi=10.1038/nm.2054|issn=1078-8956}}</ref>. Identification of del(5q) has clinical significance because patients with this cytogenetic abnormality have a good prognosis and they respond well to lenalidomide treatment. | The most characteristic cytogenetic abnormality is an interstitial deletion on the long arm of chromosome 5 or del(5q)<ref name=":0">{{Cite journal|last=Van Den Berghe|first=Herman|last2=Cassiman|first2=Jean-Jacques|last3=David|first3=Guido|last4=Fryns|first4=Jean-Pierre|last5=Michaux|first5=Jean-Louis|last6=Sokal|first6=Gerard|date=1974|title=Distinct haematological disorder with deletion of long arm of No. 5 chromosome|url=http://www.nature.com/articles/251437a0|journal=Nature|language=en|volume=251|issue=5474|pages=437–438|doi=10.1038/251437a0|issn=0028-0836}}</ref> The break point is not fixed but the region between bands q31 and q33 is generally deleted. Several candidates genes were thought to contribute to the haploinsufficiency effect of the deleted region, including ''RPS14'' <ref>{{Cite journal|last=Ebert|first=Benjamin L.|last2=Pretz|first2=Jennifer|last3=Bosco|first3=Jocelyn|last4=Chang|first4=Cindy Y.|last5=Tamayo|first5=Pablo|last6=Galili|first6=Naomi|last7=Raza|first7=Azra|last8=Root|first8=David E.|last9=Attar|first9=Eyal|date=2008|title=Identification of RPS14 as a 5q- syndrome gene by RNA interference screen|url=http://www.nature.com/articles/nature06494|journal=Nature|language=en|volume=451|issue=7176|pages=335–339|doi=10.1038/nature06494|issn=0028-0836|pmc=PMC3771855|pmid=18202658}}</ref>'', CSNK1A1'' <ref name=":1">{{Cite journal|last=Schneider|first=Rebekka K.|last2=Ademà|first2=Vera|last3=Heckl|first3=Dirk|last4=Järås|first4=Marcus|last5=Mallo|first5=Mar|last6=Lord|first6=Allegra M.|last7=Chu|first7=Lisa P.|last8=McConkey|first8=Marie E.|last9=Kramann|first9=Rafael|date=2014|title=Role of Casein Kinase 1A1 in the Biology and Targeted Therapy of del(5q) MDS|url=https://linkinghub.elsevier.com/retrieve/pii/S1535610814003353|journal=Cancer Cell|language=en|volume=26|issue=4|pages=509–520|doi=10.1016/j.ccr.2014.08.001|pmc=PMC4199102|pmid=25242043}}</ref>'','' miR-145 and miR-146a <ref>{{Cite journal|last=Starczynowski|first=Daniel T|last2=Kuchenbauer|first2=Florian|last3=Argiropoulos|first3=Bob|last4=Sung|first4=Sandy|last5=Morin|first5=Ryan|last6=Muranyi|first6=Andrew|last7=Hirst|first7=Martin|last8=Hogge|first8=Donna|last9=Marra|first9=Marco|date=2010|title=Identification of miR-145 and miR-146a as mediators of the 5q– syndrome phenotype|url=http://www.nature.com/articles/nm.2054|journal=Nature Medicine|language=en|volume=16|issue=1|pages=49–58|doi=10.1038/nm.2054|issn=1078-8956}}</ref>. Identification of del(5q) has clinical significance because patients with this cytogenetic abnormality have a good prognosis and they respond well to lenalidomide treatment. | ||
<blockquote class="blockedit"> | |||
<center><span style="color:Maroon">'''End of V4 Section'''</span> | |||
---- | |||
</blockquote> | </blockquote> | ||
==Gene Mutations (SNV / INDEL)== | ==Gene Mutations (SNV / INDEL)== | ||
| Line 296: | Line 314: | ||
<blockquote class='blockedit'>{{Box-round|title=v4:Gene Mutations (SNV/INDEL)|The content below was from the old template. Please incorporate above.}} | <blockquote class='blockedit'>{{Box-round|title=v4:Gene Mutations (SNV/INDEL)|The content below was from the old template. Please incorporate above.}}</blockquote> | ||
Somatic mutations in ''JAK2'' and ''MPL'' have been reported in a small subset patients with isolated del(5q), but these mutations seem not confer diagnostic or prognostic value <ref>{{Cite journal|last=Patnaik|first=M M|last2=Lasho|first2=T L|last3=Finke|first3=C M|last4=Gangat|first4=N|last5=Caramazza|first5=D|last6=Holtan|first6=S G|last7=Pardanani|first7=A|last8=Knudson|first8=R A|last9=Ketterling|first9=R P|date=2010|title=WHO-defined ‘myelodysplastic syndrome with isolated del(5q)’ in 88 consecutive patients: survival data, leukemic transformation rates and prevalence of JAK2, MPL and IDH mutations|url=http://www.nature.com/articles/leu2010105|journal=Leukemia|language=en|volume=24|issue=7|pages=1283–1289|doi=10.1038/leu.2010.105|issn=0887-6924|pmc=PMC3035970|pmid=20485371}}</ref>. A subset of cases could have ''[[SF3B1]]'' mutations, which needs to be differentiated with MDS-RS. | Somatic mutations in ''JAK2'' and ''MPL'' have been reported in a small subset patients with isolated del(5q), but these mutations seem not confer diagnostic or prognostic value <ref>{{Cite journal|last=Patnaik|first=M M|last2=Lasho|first2=T L|last3=Finke|first3=C M|last4=Gangat|first4=N|last5=Caramazza|first5=D|last6=Holtan|first6=S G|last7=Pardanani|first7=A|last8=Knudson|first8=R A|last9=Ketterling|first9=R P|date=2010|title=WHO-defined ‘myelodysplastic syndrome with isolated del(5q)’ in 88 consecutive patients: survival data, leukemic transformation rates and prevalence of JAK2, MPL and IDH mutations|url=http://www.nature.com/articles/leu2010105|journal=Leukemia|language=en|volume=24|issue=7|pages=1283–1289|doi=10.1038/leu.2010.105|issn=0887-6924|pmc=PMC3035970|pmid=20485371}}</ref>. A subset of cases could have ''[[SF3B1]]'' mutations, which needs to be differentiated with MDS-RS. | ||
| Line 319: | Line 337: | ||
|} | |} | ||
<blockquote class="blockedit"> | |||
<center><span style="color:Maroon">'''End of V4 Section'''</span> | |||
---- | |||
</blockquote> | </blockquote> | ||
==Epigenomic Alterations== | ==Epigenomic Alterations== | ||
| Line 344: | Line 365: | ||
|} | |} | ||
<blockquote class='blockedit'>{{Box-round|title=v4:Genes and Main Pathways Involved|The content below was from the old template. Please incorporate above.}} | <blockquote class='blockedit'>{{Box-round|title=v4:Genes and Main Pathways Involved|The content below was from the old template. Please incorporate above.}}</blockquote> | ||
Several candidate genes in the common deleted region of 5q have been reported to contribute to the molecular pathogenesis. | Several candidate genes in the common deleted region of 5q have been reported to contribute to the molecular pathogenesis. | ||
| Line 354: | Line 375: | ||
miR-145 and miR146α: These two micro RNA genes are thought to be associated with thrombocytosis and hypolobulated megakaryocytes <ref>{{Cite journal|last=Starczynowski|first=Daniel T|last2=Kuchenbauer|first2=Florian|last3=Argiropoulos|first3=Bob|last4=Sung|first4=Sandy|last5=Morin|first5=Ryan|last6=Muranyi|first6=Andrew|last7=Hirst|first7=Martin|last8=Hogge|first8=Donna|last9=Marra|first9=Marco|date=2010|title=Identification of miR-145 and miR-146a as mediators of the 5q– syndrome phenotype|url=http://www.nature.com/articles/nm.2054|journal=Nature Medicine|language=en|volume=16|issue=1|pages=49–58|doi=10.1038/nm.2054|issn=1078-8956}}</ref>. | miR-145 and miR146α: These two micro RNA genes are thought to be associated with thrombocytosis and hypolobulated megakaryocytes <ref>{{Cite journal|last=Starczynowski|first=Daniel T|last2=Kuchenbauer|first2=Florian|last3=Argiropoulos|first3=Bob|last4=Sung|first4=Sandy|last5=Morin|first5=Ryan|last6=Muranyi|first6=Andrew|last7=Hirst|first7=Martin|last8=Hogge|first8=Donna|last9=Marra|first9=Marco|date=2010|title=Identification of miR-145 and miR-146a as mediators of the 5q– syndrome phenotype|url=http://www.nature.com/articles/nm.2054|journal=Nature Medicine|language=en|volume=16|issue=1|pages=49–58|doi=10.1038/nm.2054|issn=1078-8956}}</ref>. | ||
<blockquote class="blockedit"> | |||
<center><span style="color:Maroon">'''End of V4 Section'''</span> | |||
---- | |||
</blockquote> | </blockquote> | ||
==Genetic Diagnostic Testing Methods== | ==Genetic Diagnostic Testing Methods== | ||
Revision as of 13:25, 10 February 2025
Haematolymphoid Tumours (WHO Classification, 5th ed.)
| This page is under construction |
editContent Update To WHO 5th Edition Classification Is In Process; Content Below is Based on WHO 4th Edition ClassificationThis page was converted to the new template on 2023-12-07. The original page can be found at HAEM4:Myelodysplastic Syndrome (MDS) with Isolated del(5q).
(General Instructions – The main focus of these pages is the clinically significant genetic alterations in each disease type. Use HUGO-approved gene names and symbols (italicized when appropriate), HGVS-based nomenclature for variants, as well as generic names of drugs and testing platforms or assays if applicable. Please complete tables whenever possible and do not delete them (add N/A if not applicable in the table and delete the examples); to add (or move) a row or column to a table, click within the table and select the > symbol that appears to be given options. Please do not delete or alter the section headings. The use of bullet points alongside short blocks of text rather than only large paragraphs is encouraged. Additional instructions below in italicized blue text should not be included in the final page content. Please also see Author_Instructions and FAQs as well as contact your Associate Editor or Technical Support)
Primary Author(s)*
Xiaolin Hu, Ph.D; Teresa Smolarek, Ph.D, FACMG
(q15q33).png)
WHO Classification of Disease
| Structure | Disease |
|---|---|
| Book | Haematolymphoid Tumours (5th ed.) |
| Category | Myeloid proliferations and neoplasms |
| Family | Myelodysplastic neoplasms |
| Type | Myelodysplastic neoplasms, with defining genetic abnormalities |
| Subtype(s) | Myelodysplastic neoplasm with low blasts and 5q deletion |
Definition / Description of Disease
MDS with isolated del(5q) is a type of MDS with defining cytogenetic abnormality of del(5q). The World Health Organization named it as isolated del 5q, but occasionally the deletion can occur with an additional cytogenetic abnormality other than monosomy 7 or del(7q). The 5q- syndrome was first described by Van den Berghe et al as a distinct type of MDS featured with macrocytic anemia, hypolobulated megakaryocytes, a normal or increased platelet count [1]. Deletion of 5q is the most common recurrent cytogenetic abnormality in myeloid neoplasm and it was commonly seen in 10-15% of patients with MDS[2]. A ~1.5 Mb common deleted region (CDR) at 5q32-q33 was identified in 5q- syndrome patients and was associated with good prognosis [3]. This disease has a good respond to lenalidomide treatment (See Clinical Significance).
Synonyms / Terminology
Myelodysplastic syndromes with 5q deletion; 5q minus syndrome
Epidemiology / Prevalence
- Median age 67 years [4]
- Women versus male about 2:1
Clinical Features
Put your text here and fill in the table (Instruction: Can include references in the table. Do not delete table.)
| Signs and Symptoms | EXAMPLE: Asymptomatic (incidental finding on complete blood counts)
EXAMPLE: B-symptoms (weight loss, fever, night sweats) EXAMPLE: Fatigue EXAMPLE: Lymphadenopathy (uncommon) |
| Laboratory Findings | EXAMPLE: Cytopenias
EXAMPLE: Lymphocytosis (low level) |
editv4:Clinical FeaturesThe content below was from the old template. Please incorporate above.
- Macrocytic anemia most common, usually severe and can be transfusion dependent.
- Thrombocytosis can be seen in 1/3 to 1/2 of cases, whereas thrombocytopenia or neutropenia are uncommon.
- Pancytopenia is rare. If pancytopenia with isolated 5q-, MDS with unclassifiable should be considered. [WHO]
- Good prognosis and low risk to progress to AML.
End of V4 Section
Sites of Involvement
Blood or bone marrow
Morphologic Features
On bone marrow examination, cellularity is usually normal or hypercellular. Erythroid hypoplasia may be seen. Blasts cells are < 5% in the bone marrow and < 1% in the peripheral blood. The most characteristic feature of isolated 5q- is the presence of micromegakaryocytes with hypolobated nuclei [insert pic micromegakaryocyte]. The erythroid dysplasia may be seen but not predominant. Granulocytic dysplasia is uncommon.
Hypolobated micromegakaryocytes are also seen in CML, which is characterized by leukocytosis, basophilia, and myeloid hyperplasia with leftward shift. Platelet count increase can be seen in essential thrombocythemia (ET), but ET has large megakaryocytes with hyperlobulated nuclei rather than microkaryocytes with hypolobulation in MDS with isolated del(5q).
Immunophenotype
Put your text here and fill in the table (Instruction: Can include references in the table. Do not delete table.)
| Finding | Marker |
|---|---|
| Positive (universal) | EXAMPLE: CD1 |
| Positive (subset) | EXAMPLE: CD2 |
| Negative (universal) | EXAMPLE: CD3 |
| Negative (subset) | EXAMPLE: CD4 |
editv4:ImmunophenotypeThe content below was from the old template. Please incorporate above.
There is no distinct immunophenotypic profile specific for myelodysplastic syndrome (MDS) with isolated del(5q). Currently, morphologic evaluation remains the gold standard in diagnosis of MDS. Immunophenotyping provides supportive evidence to clarify the blasts nature and percentage [5].
End of V4 Section
Chromosomal Rearrangements (Gene Fusions)
Put your text here and fill in the table
| Chromosomal Rearrangement | Genes in Fusion (5’ or 3’ Segments) | Pathogenic Derivative | Prevalence | Diagnostic Significance (Yes, No or Unknown) | Prognostic Significance (Yes, No or Unknown) | Therapeutic Significance (Yes, No or Unknown) | Notes |
|---|---|---|---|---|---|---|---|
| EXAMPLE: t(9;22)(q34;q11.2) | EXAMPLE: 3'ABL1 / 5'BCR | EXAMPLE: der(22) | EXAMPLE: 20% (COSMIC)
EXAMPLE: 30% (add reference) |
Yes | No | Yes | EXAMPLE:
The t(9;22) is diagnostic of CML in the appropriate morphology and clinical context (add reference). This fusion is responsive to targeted therapy such as Imatinib (Gleevec) (add reference). |
editv4:Chromosomal Rearrangements (Gene Fusions)The content below was from the old template. Please incorporate above.
NA
| Chromosomal Rearrangement | Genes in Fusion (5’ or 3’ Segments) | Pathogenic Derivative | Prevalence |
|---|---|---|---|
| EXAMPLE: t(9;22)(q34;q11.2) | EXAMPLE: 3'ABL1 / 5'BCR | EXAMPLE: der(22) | EXAMPLE: 5% |
| EXAMPLE: t(8;21)(q22;q22) | EXAMPLE: 5'RUNX1 / 3'RUNXT1 | EXAMPLE: der(8) | EXAMPLE: 5% |
End of V4 Section
editv4:Clinical Significance (Diagnosis, Prognosis and Therapeutic Implications).Please incorporate this section into the relevant tables found in:
- Chromosomal Rearrangements (Gene Fusions)
- Individual Region Genomic Gain/Loss/LOH
- Characteristic Chromosomal Patterns
- Gene Mutations (SNV/INDEL)
Diagnosis:
- Cytopenia in 1 to 2 lineages. Cytopenias are defined as hemoglobin concentration < 10 g/dL, platelet count < 100 x 109/L and absolute neutrophil count < 1.8 x 109/L; mild degree of anemia (hemoglobin < 13 g/dL in men or < 12 g/dL in women) or thrombocytopenia (platelets < 150 x109/L) are allowed if defining cytogenetic abnormality is present. Thrombocytosis (platelet count ≥ 450 x 109/L) is allowed in MDS with isolated del(5q). PB monocytes must be < 1 x109/L.
- Dysplasia in 1 to 3 lineages. Micromegakaryocytes with hypolobation are characteristic dysplasia. Ring sideroblasts are not common.
- Blasts percentage: BM <5%, PB <1%, no Auer rods.
- Interstitial deletion of 5q alone or with an additional abnormality other than loss of chromosome 7 or deletion of 7q.
- Chromosome 7 loss or del(7q), more than one additional cytogenetic abnormality, excess blasts need to be excluded from the diagnosis.
Prognosis:
- According to IPSS‐R good‐risk group with low rates of leukemic transformation [6].
- The median survival of MDS with isolated del(5q) is 66 to 145 months.
- About less than 10% of cases progress to acute myeloid leukemia [7].
- Mutations of TP53 may function as an independent prognostic factor in associated with leukemic progression and resistant to lenalidomide[8][9].
Therapeutic Implications:
Lenalidomide is an analogue of thalidomide which functions as an immunomodulatory agent. Treatment with lenalidomide has shown great potential in reducing the abnormal clone as well as transfusion dependency irrespective of cytogenetic complexity [10][11]. FDA approved Lenalidomide on December 2005 for treating MDS with del(5q) with or without additional cytogenetic abnormalities.
End of V4 Section
Individual Region Genomic Gain / Loss / LOH
Put your text here and fill in the table (Instructions: Includes aberrations not involving gene fusions. Can include references in the table. Can refer to CGC workgroup tables as linked on the homepage if applicable. Do not delete table.)
| Chr # | Gain / Loss / Amp / LOH | Minimal Region Genomic Coordinates [Genome Build] | Minimal Region Cytoband | Diagnostic Significance (Yes, No or Unknown) | Prognostic Significance (Yes, No or Unknown) | Therapeutic Significance (Yes, No or Unknown) | Notes |
|---|---|---|---|---|---|---|---|
| EXAMPLE:
7 |
EXAMPLE: Loss | EXAMPLE:
chr7:1- 159,335,973 [hg38] |
EXAMPLE:
chr7 |
Yes | Yes | No | EXAMPLE:
Presence of monosomy 7 (or 7q deletion) is sufficient for a diagnosis of AML with MDS-related changes when there is ≥20% blasts and no prior therapy (add reference). Monosomy 7/7q deletion is associated with a poor prognosis in AML (add reference). |
| EXAMPLE:
8 |
EXAMPLE: Gain | EXAMPLE:
chr8:1-145,138,636 [hg38] |
EXAMPLE:
chr8 |
No | No | No | EXAMPLE:
Common recurrent secondary finding for t(8;21) (add reference). |
editv4:Genomic Gain/Loss/LOHThe content below was from the old template. Please incorporate above.
| Chromosome Number | Gain/Loss/Amp/LOH | Region |
|---|---|---|
| EXAMPLE: 8 | EXAMPLE: Gain | EXAMPLE: chr8:0-1000000 |
| EXAMPLE: 7 | EXAMPLE: Loss | EXAMPLE: chr7:0-1000000 |
End of V4 Section
Characteristic Chromosomal Patterns
Put your text here (EXAMPLE PATTERNS: hyperdiploid; gain of odd number chromosomes including typically chromosome 1, 3, 5, 7, 11, and 17; co-deletion of 1p and 19q; complex karyotypes without characteristic genetic findings; chromothripsis. Do not delete table.)
| Chromosomal Pattern | Diagnostic Significance (Yes, No or Unknown) | Prognostic Significance (Yes, No or Unknown) | Therapeutic Significance (Yes, No or Unknown) | Notes |
|---|---|---|---|---|
| EXAMPLE:
Co-deletion of 1p and 18q |
Yes | No | No | EXAMPLE:
See chromosomal rearrangements table as this pattern is due to an unbalanced derivative translocation associated with oligodendroglioma (add reference). |
editv4:Characteristic Chromosomal Aberrations / PatternsThe content below was from the old template. Please incorporate above.
The most characteristic cytogenetic abnormality is an interstitial deletion on the long arm of chromosome 5 or del(5q)[1] The break point is not fixed but the region between bands q31 and q33 is generally deleted. Several candidates genes were thought to contribute to the haploinsufficiency effect of the deleted region, including RPS14 [12], CSNK1A1 [13], miR-145 and miR-146a [14]. Identification of del(5q) has clinical significance because patients with this cytogenetic abnormality have a good prognosis and they respond well to lenalidomide treatment.
End of V4 Section
Gene Mutations (SNV / INDEL)
Put your text here and fill in the table (Instructions: This table is not meant to be an exhaustive list; please include only genes/alterations that are recurrent and common as well as either disease defining and/or clinically significant. Can include references in the table. For clinical significance, denote associations with FDA-approved therapy (not an extensive list of applicable drugs) and NCCN or other national guidelines if applicable. Can also refer to CGC workgroup tables as linked on the homepage if applicable as well as any high impact papers or reviews of gene mutations in this entity. Do not delete table.)
| Gene; Genetic Alteration | Presumed Mechanism (Tumor Suppressor Gene [TSG] / Oncogene / Other) | Prevalence (COSMIC / TCGA / Other) | Concomitant Mutations | Mutually Exclusive Mutations | Diagnostic Significance (Yes, No or Unknown) | Prognostic Significance (Yes, No or Unknown) | Therapeutic Significance (Yes, No or Unknown) | Notes |
|---|---|---|---|---|---|---|---|---|
| EXAMPLE: TP53; Variable LOF mutations
EXAMPLE: EGFR; Exon 20 mutations EXAMPLE: BRAF; Activating mutations |
EXAMPLE: TSG | EXAMPLE: 20% (COSMIC)
EXAMPLE: 30% (add Reference) |
EXAMPLE: IDH1 R123H | EXAMPLE: EGFR amplification | EXAMPLE: Excludes hairy cell leukemia (HCL) (add reference).
|
Note: A more extensive list of mutations can be found in cBioportal (https://www.cbioportal.org/), COSMIC (https://cancer.sanger.ac.uk/cosmic), ICGC (https://dcc.icgc.org/) and/or other databases. When applicable, gene-specific pages within the CCGA site directly link to pertinent external content.
editv4:Gene Mutations (SNV/INDEL)The content below was from the old template. Please incorporate above.
Somatic mutations in JAK2 and MPL have been reported in a small subset patients with isolated del(5q), but these mutations seem not confer diagnostic or prognostic value [15]. A subset of cases could have SF3B1 mutations, which needs to be differentiated with MDS-RS.
| Gene | Mutation | Oncogene/Tumor Suppressor/Other | Presumed Mechanism (LOF/GOF/Other; Driver/Passenger) | Prevalence (COSMIC/TCGA/Other) |
|---|---|---|---|---|
| EXAMPLE: TP53 | EXAMPLE: R273H | EXAMPLE: Tumor Suppressor | EXAMPLE: LOF | EXAMPLE: 20% |
Other Mutations
| Type | Gene/Region/Other |
|---|---|
| Concomitant Mutations | JAK2 V617F, MPL W515L |
| Secondary Mutations | |
| Mutually Exclusive |
End of V4 Section
Epigenomic Alterations
Genes involved in epigenetic regulation are frequently mutated in MDS such as TET2, DNMT3A, IDH1, IDH2, AXSL1, and EZH2 [16]. These genes play a role in DNA methylation and chromatin modification as well as regulating gene expression.
Genes and Main Pathways Involved
Put your text here and fill in the table (Instructions: Can include references in the table. Do not delete table.)
| Gene; Genetic Alteration | Pathway | Pathophysiologic Outcome |
|---|---|---|
| EXAMPLE: BRAF and MAP2K1; Activating mutations | EXAMPLE: MAPK signaling | EXAMPLE: Increased cell growth and proliferation |
| EXAMPLE: CDKN2A; Inactivating mutations | EXAMPLE: Cell cycle regulation | EXAMPLE: Unregulated cell division |
| EXAMPLE: KMT2C and ARID1A; Inactivating mutations | EXAMPLE: Histone modification, chromatin remodeling | EXAMPLE: Abnormal gene expression program |
editv4:Genes and Main Pathways InvolvedThe content below was from the old template. Please incorporate above.
Several candidate genes in the common deleted region of 5q have been reported to contribute to the molecular pathogenesis.
RPS14: Encodes for ribosomal subunit of 40S. Inactivation of RPS14 results in ineffective erythroid differentiation and increased apoptosis in a p53 dependent way [17].
CSNK1A1: Encodes for CK1α, a serine/threonine protein kinase activity. Mutations in CSNK1A1 lead to clonal expansion of hematopoietic stem cells through activation of β-catenin [13].
miR-145 and miR146α: These two micro RNA genes are thought to be associated with thrombocytosis and hypolobulated megakaryocytes [18].
End of V4 Section
Genetic Diagnostic Testing Methods
- Bone marrow morphology and peripheral blood test are standard in diagnosis of MDS.
- FISH probes targeting the CDR are commonly incorporated into MDS panel to assess -5/5q-.
- Conventional cytogenetics are also helpful in diagnosis.
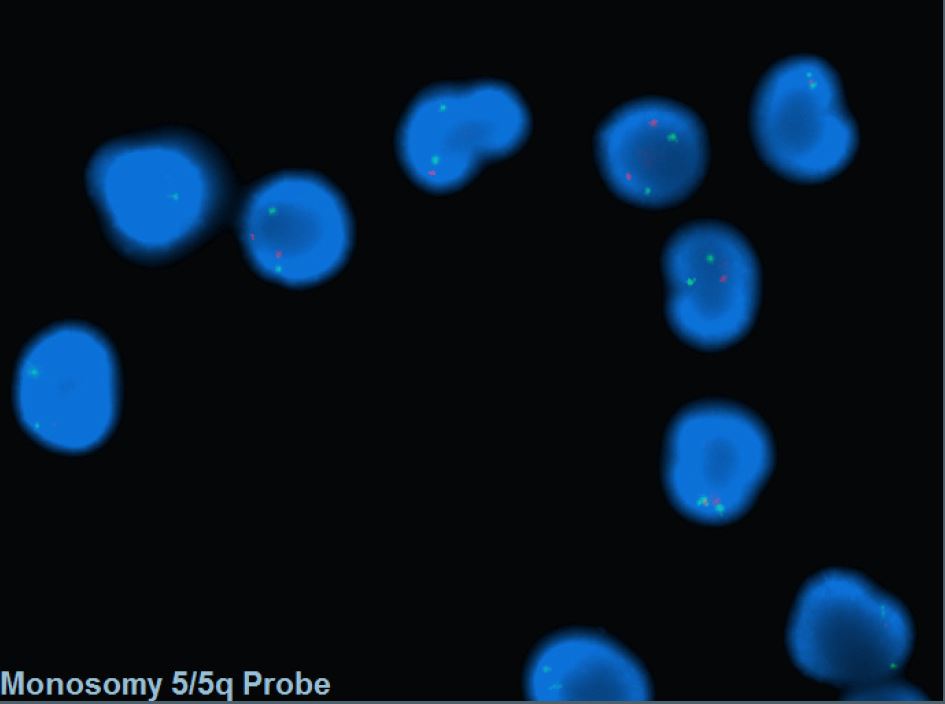
Fluorescent in situ hybridization (FISH) with a dual color DNA probe specific for the EGR1 (5q31.2) locus and to a distal short arm locus (5p15.31) of chromosome 5 detected two green and one red signal pattern that consistents with 5q deletion in 51% of patient's cells.

Familial Forms
Put your text here (Instructions: Include associated hereditary conditions/syndromes that cause this entity or are caused by this entity.)
Additional Information
Put your text here
Links
Put your links here (use link icon at top of page)
References
(use the "Cite" icon at the top of the page) (Instructions: Add each reference into the text above by clicking on where you want to insert the reference, selecting the “Cite” icon at the top of the page, and using the “Automatic” tab option to search such as by PMID to select the reference to insert. The reference list in this section will be automatically generated and sorted. If a PMID is not available, such as for a book, please use the “Cite” icon, select “Manual” and then “Basic Form”, and include the entire reference.)
- ↑ 1.0 1.1 Van Den Berghe, Herman; et al. (1974). "Distinct haematological disorder with deletion of long arm of No. 5 chromosome". Nature. 251 (5474): 437–438. doi:10.1038/251437a0. ISSN 0028-0836.
- ↑ Hosono, Naoko; et al. (2017). "Recurrent genetic defects on chromosome 5q in myeloid neoplasms". Oncotarget. 8 (4): 6483–6495. doi:10.18632/oncotarget.14130. ISSN 1949-2553. PMC 5351647. PMID 28031539.CS1 maint: PMC format (link)
- ↑ Boultwood, J.; et al. (1994). "Molecular Mapping of Uncharacteristically Small 5q Deletions in Two Patients with the 5q- Syndrome: Delineation of the Critical Region on 5q and Identification of a 5q- Breakpoint". Genomics. 19 (3): 425–432. doi:10.1006/geno.1994.1090.
- ↑ Giagounidis, A.A.N.; et al. (2004). "Hematological Malignancies". Hematology. 9 (4): 271–277. doi:10.1080/10245330410001723824. ISSN 1607-8454.
- ↑ Zini, Gina (2017). "Diagnostics and Prognostication of Myelodysplastic Syndromes". Annals of Laboratory Medicine. 37 (6): 465. doi:10.3343/alm.2017.37.6.465. ISSN 2234-3806. PMC 5587818. PMID 28840983.CS1 maint: PMC format (link)
- ↑ Mallo, M; et al. (2011). "Impact of adjunct cytogenetic abnormalities for prognostic stratification in patients with myelodysplastic syndrome and deletion 5q". Leukemia. 25 (1): 110–120. doi:10.1038/leu.2010.231. ISSN 0887-6924.
- ↑ Boultwood, Jacqueline; et al. (2010). "Advances in the 5q− syndrome". Blood. 116 (26): 5803–5811. doi:10.1182/blood-2010-04-273771. ISSN 0006-4971.
- ↑ Jädersten, Martin; et al. (2011). "TP53 Mutations in Low-Risk Myelodysplastic Syndromes With del(5q) Predict Disease Progression". Journal of Clinical Oncology. 29 (15): 1971–1979. doi:10.1200/JCO.2010.31.8576. ISSN 0732-183X.
- ↑ Kulasekararaj, Austin G.; et al. (2013). "TP53 mutations in myelodysplastic syndrome are strongly correlated with aberrations of chromosome 5, and correlate with adverse prognosis". British Journal of Haematology. 160 (5): 660–672. doi:10.1111/bjh.12203.
- ↑ Giagounidis, A. A. N.; et al. (2005). "Prognosis of patients with del(5q) MDS and complex karyotype and the possible role of lenalidomide in this patient subgroup". Annals of Hematology. 84 (9): 569–571. doi:10.1007/s00277-005-1054-0. ISSN 0939-5555.
- ↑ List, Alan; et al. (2006). "Lenalidomide in the Myelodysplastic Syndrome with Chromosome 5q Deletion". New England Journal of Medicine. 355 (14): 1456–1465. doi:10.1056/NEJMoa061292. ISSN 0028-4793.
- ↑ Ebert, Benjamin L.; et al. (2008). "Identification of RPS14 as a 5q- syndrome gene by RNA interference screen". Nature. 451 (7176): 335–339. doi:10.1038/nature06494. ISSN 0028-0836. PMC 3771855. PMID 18202658.CS1 maint: PMC format (link)
- ↑ 13.0 13.1 Schneider, Rebekka K.; et al. (2014). "Role of Casein Kinase 1A1 in the Biology and Targeted Therapy of del(5q) MDS". Cancer Cell. 26 (4): 509–520. doi:10.1016/j.ccr.2014.08.001. PMC 4199102. PMID 25242043.CS1 maint: PMC format (link)
- ↑ Starczynowski, Daniel T; et al. (2010). "Identification of miR-145 and miR-146a as mediators of the 5q– syndrome phenotype". Nature Medicine. 16 (1): 49–58. doi:10.1038/nm.2054. ISSN 1078-8956.
- ↑ Patnaik, M M; et al. (2010). "WHO-defined 'myelodysplastic syndrome with isolated del(5q)' in 88 consecutive patients: survival data, leukemic transformation rates and prevalence of JAK2, MPL and IDH mutations". Leukemia. 24 (7): 1283–1289. doi:10.1038/leu.2010.105. ISSN 0887-6924. PMC 3035970. PMID 20485371.CS1 maint: PMC format (link)
- ↑ Heuser, Michael; et al. (2018). "Epigenetics in myelodysplastic syndromes". Seminars in Cancer Biology. 51: 170–179. doi:10.1016/j.semcancer.2017.07.009.
- ↑ Barlow, Jillian L; et al. (2010). "A p53-dependent mechanism underlies macrocytic anemia in a mouse model of human 5q– syndrome". Nature Medicine. 16 (1): 59–66. doi:10.1038/nm.2063. ISSN 1078-8956. PMC 2803774. PMID 19966810.CS1 maint: PMC format (link)
- ↑ Starczynowski, Daniel T; et al. (2010). "Identification of miR-145 and miR-146a as mediators of the 5q– syndrome phenotype". Nature Medicine. 16 (1): 49–58. doi:10.1038/nm.2054. ISSN 1078-8956.
Notes
*Primary authors will typically be those that initially create and complete the content of a page. If a subsequent user modifies the content and feels the effort put forth is of high enough significance to warrant listing in the authorship section, please contact the CCGA coordinators (contact information provided on the homepage). Additional global feedback or concerns are also welcome. *Citation of this Page: “Myelodysplastic neoplasm with low blasts and 5q deletion”. Compendium of Cancer Genome Aberrations (CCGA), Cancer Genomics Consortium (CGC), updated 02/10/2025, https://ccga.io/index.php/HAEM5:Myelodysplastic_neoplasm_with_low_blasts_and_5q_deletion.