Intrachromosomal amplification of chromosome 21 (iAMP21) is a neoplasm of lymphoblasts that are of the B-cell lineage. It is characterized by amplification of the RUNX1 gene at 21q22.3 on a structurally abnormal chromosome 21. Amplification is defined as ≥5 copies of RUNX1 detected by FISH or ≥3 copies of RUNX1 on a single abnormal chromosome 21.[1]
Synonyms / Terminology
Put your text here (Instructions: Include currently used terms and major historical ones, adding “(historical)” after the latter.)
Epidemiology / Prevalence
iAMP21 is observed most often in the older pediatric group (median age of 9 years, with a range of 2-30 years). It accounts for ~2% of B-ALL cases including ~2% of standard-risk and 3% of high-risk patients. The incidence in adult B-ALL has not been established; however, it appears to be less prevalent than in the pediatric population.[2]
Further, patients carrying a rob(15;21)(q10;q10) have an ~2700-fold increased risk of developing iAMP21 ALL compared to the general population. Additionally, patients with a constitutional ring chromosome 21, r(21), may potentially be predisposed to iAMP21 ALL.[2]
Clinical Features
Put your text here and fill in the table (Instruction: Can include references in the table)
Signs and Symptoms
EXAMPLE Asymptomatic (incidental finding on complete blood counts)
EXAMPLE B-symptoms (weight loss, fever, night sweats)
The content below was from the old template. Please incorporate above.
Patients tend to present with a low platelet count and low WBC count (<50,000/µl). ~50% of cases are classified as high-risk based on an age of ≥10 years.[3]
Sites of Involvement
Bone Marrow and peripheral blood
Morphologic Features
There are no unique morphological or cytochemical features that distinguish this entity from other types of ALL.[1]
Cytogenetic morphology of the abnormal chromosome 21 can vary markedly between patients.[4]
iAMP21 in a ring formation; Courtesy of Fullerton Genetics Lab
Immunophenotype
No detailed information is known, other than these cases occur exclusively in B-ALL.[1]
Finding
Marker
Positive (universal)
EXAMPLE CD1
Positive (subset)
EXAMPLE CD2
Negative (universal)
EXAMPLE CD3
Negative (subset)
EXAMPLE CD4
Chromosomal Rearrangements (Gene Fusions)
Put your text here and fill in the table
Chromosomal Rearrangement
Genes in Fusion (5’ or 3’ Segments)
Pathogenic Derivative
Prevalence
Diagnostic Significance (Yes, No or Unknown)
Prognostic Significance (Yes, No or Unknown)
Therapeutic Significance (Yes, No or Unknown)
Notes
EXAMPLE t(9;22)(q34;q11.2)
EXAMPLE 3'ABL1 / 5'BCR
EXAMPLE der(22)
EXAMPLE 20% (COSMIC)
EXAMPLE 30% (add reference)
Yes
No
Yes
EXAMPLE
The t(9;22) is diagnostic of CML in the appropriate morphology and clinical context (add reference). This fusion is responsive to targeted therapy such as Imatinib (Gleevec) (add reference).
The content below was from the old template. Please incorporate above.
Some rearrangements have been seen as secondary abnormalities.
Chromosomal Rearrangement
Genes in Fusion (5’ or 3’ Segments)
Pathogenic Derivative
Prevalence
del(X)(p22.33p22.33)/del(Y)(p11.32p11.32)
P2RY8-CRLF2
der(X)/der(Y)
t(12;21)(p13.2;q22.1)
ETV6-RUNX1
der(21)
t(9;22)(q34;q11.2)
BCR-ABL1
der(22)
editv4:Clinical Significance (Diagnosis, Prognosis and Therapeutic Implications).
Please incorporate this section into the relevant tables found in:
Chromosomal Rearrangements (Gene Fusions)
Individual Region Genomic Gain/Loss/LOH
Characteristic Chromosomal Patterns
Gene Mutations (SNV/INDEL)
Pediatric iAMP21 has been associated with a poor outcome. It displays an increased rate of relapse when treated on standard protocols. Further, the event-free survival and overall survival were significantly worse for individuals with the iAMP21 and standard-risk B-ALL, but not significant in individuals with iAMP21 and high-risk B-ALL.
Because of the unique nature of the iAMP21 abnormality, cases that present with additional genomic lesions that may suggest another category, such as a CRLF2 rearrangement, should still be classified as B-ALL with iAMP21.
Individual Region Genomic Gain / Loss / LOH
Put your text here and fill in the table (Instructions: Includes aberrations not involving gene fusions. Can include references in the table. Can refer to CGC workgroup tables as linked on the homepage if applicable.)
Chr #
Gain / Loss / Amp / LOH
Minimal Region Genomic Coordinates [Genome Build]
Minimal Region Cytoband
Diagnostic Significance (Yes, No or Unknown)
Prognostic Significance (Yes, No or Unknown)
Therapeutic Significance (Yes, No or Unknown)
Notes
EXAMPLE
7
EXAMPLE Loss
EXAMPLE
chr7:1- 159,335,973 [hg38]
EXAMPLE
chr7
Yes
Yes
No
EXAMPLE
Presence of monosomy 7 (or 7q deletion) is sufficient for a diagnosis of AML with MDS-related changes when there is ≥20% blasts and no prior therapy (add reference). Monosomy 7/7q deletion is associated with a poor prognosis in AML (add reference).
EXAMPLE
8
EXAMPLE Gain
EXAMPLE
chr8:1-145,138,636 [hg38]
EXAMPLE
chr8
No
No
No
EXAMPLE
Common recurrent secondary finding for t(8;21) (add reference).
The content below was from the old template. Please incorporate above.
In ~80% of iAMP21 B-ALL cases, recurrent secondary abnormalities, both chromosomal and molecular, have been documented. Deletions involving particular genes such as; IKZF1, CDKN2A/B, PAX5, SH2B3, ETV6 and RB1 have also been observed.
Chromosome Number
Gain/Loss/Amp/LOH
X
Gain
10
Gain
14
Gain
7/7q
Loss
11q
Loss
Characteristic Chromosomal Patterns
Put your text here (EXAMPLE PATTERNS: hyperdiploid; gain of odd number chromosomes including typically chromosome 1, 3, 5, 7, 11, and 17; co-deletion of 1p and 19q; complex karyotypes without characteristic genetic findings; chromothripsis)
Chromosomal Pattern
Diagnostic Significance (Yes, No or Unknown)
Prognostic Significance (Yes, No or Unknown)
Therapeutic Significance (Yes, No or Unknown)
Notes
EXAMPLE
Co-deletion of 1p and 18q
Yes
No
No
EXAMPLE:
See chromosomal rearrangements table as this pattern is due to an unbalanced derivative translocation associated with oligodendroglioma (add reference).
The content below was from the old template. Please incorporate above.
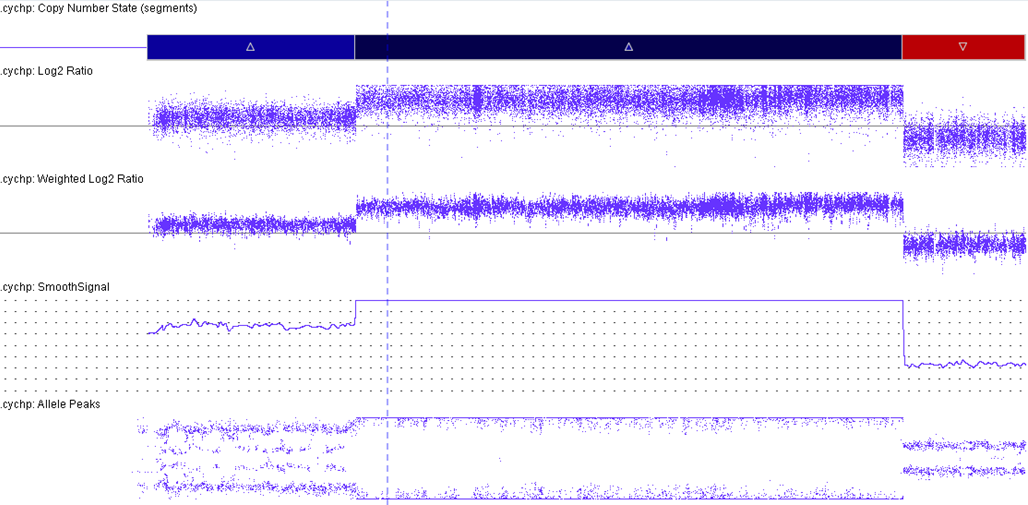
Characteristic iAMP21 CMA; Courtesy of Fullerton Genetics Lab
iAMP21 cases have a characteristic pattern that is both complex and variable. This pattern comprises multiple regions of gain, amplification and deletion. Further, it often is accompanied by a terminal deletion of 21q. Interestingly, RUNX1 amplification is not always intrachromosomal.[5][6]
The formation of iAMP21 is considered to be due to breakage-fusion-bridge cycles followed by chromothripsis and other complex structural rearrangements of chromosome 21. Studies, molecular and cytogenetic, have elucidated a common 5.1 Mb region that includes the RUNX1 gene. This is part of the critical region consistently amplified (chr21:32.8-37.9 Mb, GRCh37/hg19). However, even though RUNX1 is included in the amplified region, there has not yet been any conclusive evidence that RUNX1 is critical in the pathogenesis of disease given that it is not overexpressed in some individuals with this abnormality.[2][7][8]
Gene Mutations (SNV / INDEL)
Put your text here and fill in the table (Instructions: This table is not meant to be an exhaustive list; please include only genes/alterations that are recurrent and common as well either disease defining and/or clinically significant. Can include references in the table. For clinical significance, denote associations with FDA-approved therapy (not an extensive list of applicable drugs) and NCCN or other national guidelines if applicable; Can also refer to CGC workgroup tables as linked on the homepage if applicable as well as any high impact papers or reviews of gene mutations in this entity.)
The content below was from the old template. Please incorporate above.
In a 2016 paper, it was shown that in the iAMP21-ALL exome, the mutations were more commonly transitions (for example: C>T) than transversions or indels.[2][9] Frequently, mutations in the RAS signaling pathway have been observed. Interestingly, these mutations were observed to coexist in patterns ranging from 2-3 mutated genes to 2-4 mutations in the same gene in one sample. Further, the FLT3-ITD was more prevalent in iAMP21-ALL.[9]
Put your links here (use "Link" icon at top of page)
References
(use the "Cite" icon at the top of the page) (Instructions: Add each reference into the text above by clicking on where you want to insert the reference, selecting the “Cite” icon at the top of the page, and using the “Automatic” tab option to search such as by PMID to select the reference to insert. The reference list in this section will be automatically generated and sorted.If a PMID is not available, such as for a book, please use the “Cite” icon, select “Manual” and then “Basic Form”, and include the entire reference.)
↑ 1.01.11.2Borowitz MJ, et al., (2017). B-Lymphoblastic leukaemia/lymphoma with recurrent genetic abnormalities, in World Health Organization Classification of Tumours of Haematopoietic and Lymphoid Tissues, Revised 4th edition. Swerdlow SH, Campo E, Harris NL, Jaffe ES, Pileri SA, Stein H, Thiele J, Arber DA, Hasserjian RP, Le Beau MM, Orazi A, and Siebert R, Editors. IARC Press: Lyon, France.
*Primary authors will typically be those that initially create and complete the content of a page. If a subsequent user modifies the content and feels the effort put forth is of high enough significance to warrant listing in the authorship section, please contact the CCGA coordinators (contact information provided on the homepage). Additional global feedback or concerns are also welcome.
*Citation of this Page: “B-lymphoblastic leukaemia/lymphoma with iAMP21”. Compendium of Cancer Genome Aberrations (CCGA), Cancer Genomics Consortium (CGC), updated 12/4/2023, https://ccga.io/index.php/HAEM5:B-lymphoblastic_leukaemia/lymphoma_with_iAMP21.