Revision as of 14:09, 3 November 2023 by Bailey.Glen(talk | contribs)(Created page with "{{DISPLAYTITLE:Plasmablastic lymphoma}} Haematolymphoid Tumours (5th ed.) {{Under Construction}} <blockquote class='blockedit'>{{Box-round|title=...")
In 1997, Delecluse et al. described a series of large B-cell lymphomas occurring within the jaw and oral cavities of HIV-positive individuals[1]. The cells were blastic in appearance and did not express CD20, but did demonstrate plasmacytic antigens. Plasmablastic lymphoma (PBL) is recognized by the World Health Organization (WHO) as an aggressive proliferation of large B cells with immunoblastic or plasmablastic morphology and plasmacytic phenotype[2]. This entity is distinguished from other large B-cell lymphomas with similar immunoprofiles, such as ALK-positive large B-cell lymphoma and HHV-8-associated lymphoproliferative disorders.
Synonyms / Terminology
Monomorphic plasmablastic lymphoma; plasmablastic lymphoma with plasmacytic differentiation
Epidemiology / Prevalence
Plasmablastic lymphoma typically occurs in adults with human immunodeficiency virus (HIV) infection (approximately 73% of cases)[3].
It is also seen in the setting of iatrogenic immunosuppression (autoimmune disease or post-transplant)[4].
PBL has been observed in older immunocompetent adults and in children, typically with HIV or immunodeficiency[5][6].
Clinical Features
Put your text here and fill in the table (Instruction: Can include references in the table)
Signs and Symptoms
EXAMPLE Asymptomatic (incidental finding on complete blood counts)
EXAMPLE B-symptoms (weight loss, fever, night sweats)
The content below was from the old template. Please incorporate above.
An extranodal mass is the most typical presentation, and nodal disease is more common in post-transplant PBL[3]. Paraproteins may be detected in some cases[7]. Greater than 50% of cases associated with some form of immunodeficiency present with stage III/IV disease with bone marrow involvement[3][5].
Sites of Involvement
Typically head and neck regions, particularly the oral cavity. Other less commonly involved sites include the gastrointestinal tract, skin, soft tissue, lung, bone, and rarely lymph nodes[8].
(PBL, monomorphic variant; image courtesy of Mark Evans, MD)
Morphologic Features
Two histologic variants have been described:
The monomorphic variant features large immunoblast-like cells with fine nuclear chromatin, prominent nucleoli, and little or no plasmacytic differentiation; a starry sky pattern is common.
The variant with plasmacytic differentiation is composed of cells with course nuclear chromatin, basophilic cytoplasm, eccentric nuclei, and paranuclear hof.
Some cases demonstrate features of both variants[2].
Immunophenotype
Put your text here and fill in the table (Instruction: Can include references in the table)
The content below was from the old template. Please incorporate above.
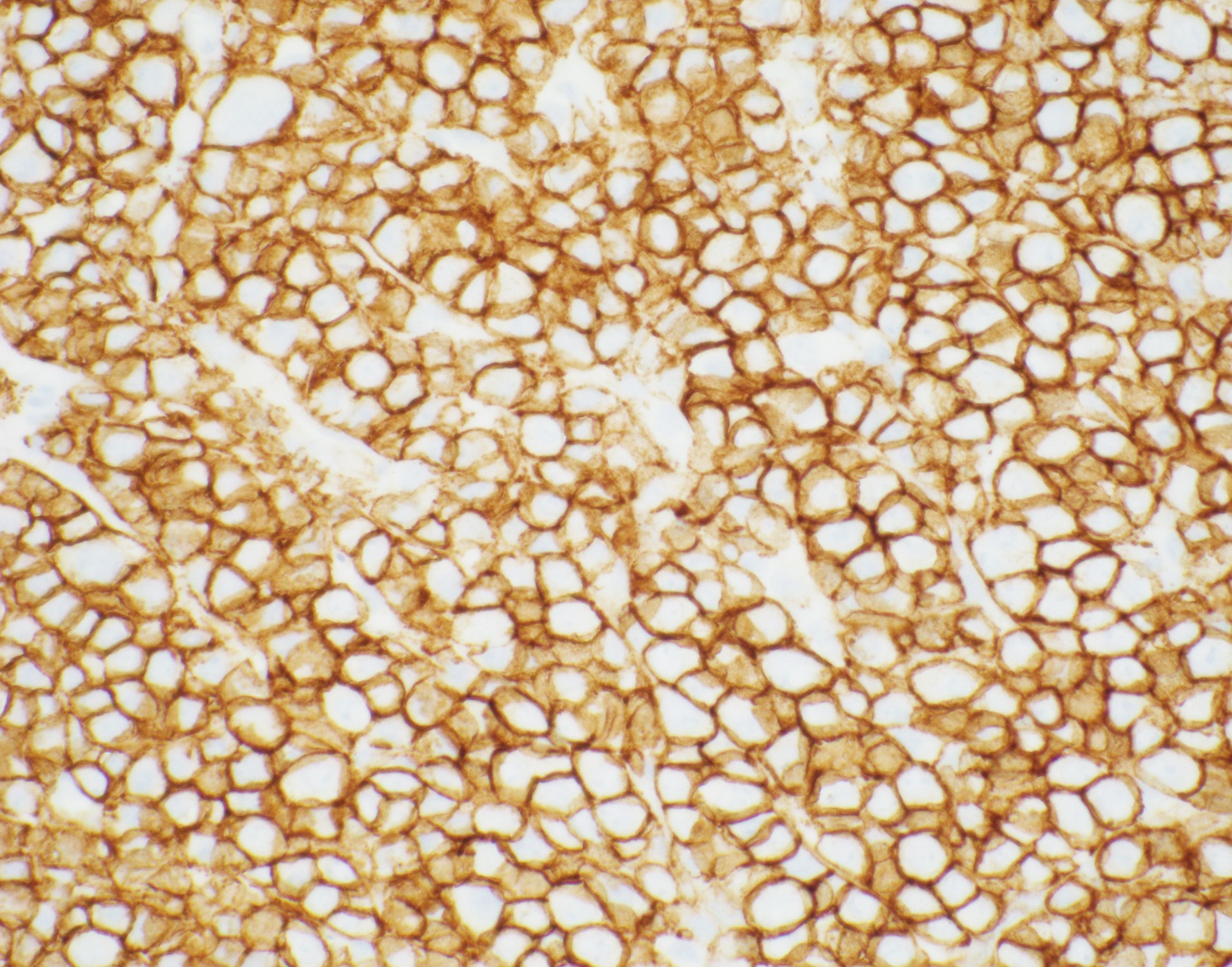
(PBL strongly positive for CD138 by immunohistochemistry; image courtesy of Mark Evans, MD)
The cells express plasmacytic antigens (CD138, VS38c, IRF4/MUM1, BLIMP1, XBP1, and CD38). CD45, PAX-5, and CD20 are typically negative or weakly positive. Cytoplasmic IgG, as well as kappa and lambda light chains are common. CD79a is present in approximately 40% of cases, and CD56 in about 25%. The cells are typically positive for Epstein-Barr virus-encoded RNA (EBER). Ki-67 proliferation index is usually >90%[8][9].
Chromosomal Rearrangements (Gene Fusions)
Put your text here and fill in the table
Chromosomal Rearrangement
Genes in Fusion (5’ or 3’ Segments)
Pathogenic Derivative
Prevalence
Diagnostic Significance (Yes, No or Unknown)
Prognostic Significance (Yes, No or Unknown)
Therapeutic Significance (Yes, No or Unknown)
Notes
EXAMPLE t(9;22)(q34;q11.2)
EXAMPLE 3'ABL1 / 5'BCR
EXAMPLE der(22)
EXAMPLE 20% (COSMIC)
EXAMPLE 30% (add reference)
Yes
No
Yes
EXAMPLE
The t(9;22) is diagnostic of CML in the appropriate morphology and clinical context (add reference). This fusion is responsive to targeted therapy such as Imatinib (Gleevec) (add reference).
The content below was from the old template. Please incorporate above.
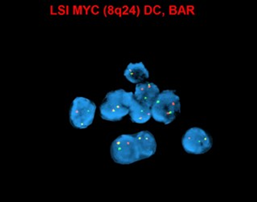
MYC (8q24) up-regulation occurs via translocations, frequently between MYC and immunoglobulin (IG) heavy chain [t(8;14)] and immunoglobulin light chain genes [t(2;8) or t(8;22)], which are also seen in Burkitt lymphoma. These translocations are more common in EBV-positive tumors (74%), and have been associated with poorer prognosis[10][11].
(Rearrangement of MYC by FISH (yellow signals); image courtesy of Fabiola Quintero-Rivera, MD)
editv4:Clinical Significance (Diagnosis, Prognosis and Therapeutic Implications).
Please incorporate this section into the relevant tables found in:
Chromosomal Rearrangements (Gene Fusions)
Individual Region Genomic Gain/Loss/LOH
Characteristic Chromosomal Patterns
Gene Mutations (SNV/INDEL)
The prognosis of PBL is very poor, with three quarters of patients dying with a median survival of 6-11 months[3][12].
There is currently no standard therapy for PBL. CHOP (cyclophosphamide, doxorubicin, vincristine, and prednisone) have been generally considered inadequate, and the National Comprehensive Cancer Network (NCCN) favors Hyper-CVAD-MA (hyperfractionated cyclophosphamide, vincristine, doxorubicin, dexamethasone, and high-dose methotrexate and cytarabine), CODOX-M/IVAC (cyclophosphamide, vincristine, doxorubicin, high-dose methotrexate/ifosfamide, etoposide, and high-dose cytarabine), COMB (cyclophosphamide, Oncovin, methyl-CCNU, and bleomycin), and infusional EPOCH (etoposide, prednisone, vincristine, cyclophosphamide, and doxorubicin)[11][13][14].
Patients with localized disease have a better prognosis, and these individuals can be managed by radiotherapy and doxorubicin-based chemotherapy with radiation therapy[15][16].
Polychemotherapy is required for patients with disseminated disease; more than 50% achieve complete remissions (CRs), but approximately 70% die of progressive disease, with an event-free survival of 22 months, and an overall survival of 32 months[17].
Individual Region Genomic Gain/Loss/LOH
Put your text here and fill in the table (Instructions: Includes aberrations not involving gene fusions. Can include references in the table. Can refer to CGC workgroup tables as linked on the homepage if applicable.)
Chr #
Gain / Loss / Amp / LOH
Minimal Region Genomic Coordinates [Genome Build]
Minimal Region Cytoband
Diagnostic Significance (Yes, No or Unknown)
Prognostic Significance (Yes, No or Unknown)
Therapeutic Significance (Yes, No or Unknown)
Notes
EXAMPLE
7
EXAMPLE Loss
EXAMPLE
chr7:1- 159,335,973 [hg38]
EXAMPLE
chr7
Yes
Yes
No
EXAMPLE
Presence of monosomy 7 (or 7q deletion) is sufficient for a diagnosis of AML with MDS-related changes when there is ≥20% blasts and no prior therapy (add reference). Monosomy 7/7q deletion is associated with a poor prognosis in AML (add reference).
EXAMPLE
8
EXAMPLE Gain
EXAMPLE
chr8:1-145,138,636 [hg38]
EXAMPLE
chr8
No
No
No
EXAMPLE
Common recurrent secondary finding for t(8;21) (add reference).
The content below was from the old template. Please incorporate above.
One study of 12 PBL cases showed recurrent gains of 1q31.1q44, 5p15.33p13.1, 7q11.2q11.23, 8q24.13q24.3, 11p and 11q terminal regions, 15q15q26.3, 19p13.3p13.12 and chromosomes 3, 7, 11, and 15, as well as losses of 1p36.33p35.1, 6q25.1q27, 8p23.3p22.14 and 18q21.32q23. Additionally, 54% of the cases had either deletion or copy neutral loss of heterozygosity (CN-LOH) involving the tumor suppressor gene CDKN2C at 1p32.3. Furthermore, recurrent copy number losses involving the immunoglobulin genes IGH and IGKV were documented[18].
(Reciprocal translocation between the MYC and IGH loci by FISH (yellow signals); image courtesy of Fabiola Quintero-Rivera, MD)
Characteristic Chromosomal Patterns
Put your text here (EXAMPLE PATTERNS: hyperdiploid; gain of odd number chromosomes including typically chromosome 1, 3, 5, 7, 11, and 17; co-deletion of 1p and 19q; complex karyotypes without characteristic genetic findings; chromothripsis)
Chromosomal Pattern
Diagnostic Significance (Yes, No or Unknown)
Prognostic Significance (Yes, No or Unknown)
Therapeutic Significance (Yes, No or Unknown)
Notes
EXAMPLE
Co-deletion of 1p and 18q
Yes
No
No
EXAMPLE:
See chromosomal rearrangements table as this pattern is due to an unbalanced derivative translocation associated with oligodendroglioma (add reference).
The content below was from the old template. Please incorporate above.
In addition to the MYC/IG rearrangements, complex karyotypes are also frequently observed. PBL often demonstrates chromosomal changes seen in plasma cell myeloma, including gain of 1q, loss of 1p, deletions 13q and/or 17p, and gains of odd-numbered chromosomes, such as +3, +5, +7, +9, +11, and/or +15[7][19].
Gene Mutations (SNV/INDEL)
Put your text here and fill in the table (Instructions: This table is not meant to be an exhaustive list; please include only genes/alterations that are recurrent and common as well either disease defining and/or clinically significant. Can include references in the table. For clinical significance, denote associations with FDA-approved therapy (not an extensive list of applicable drugs) and NCCN or other national guidelines if applicable; Can also refer to CGC workgroup tables as linked on the homepage if applicable as well as any high impact papers or reviews of gene mutations in this entity.)
The content below was from the old template. Please incorporate above.
IGHV may be unmutated or demonstrate somatic hypermutation[20].
Montes-Moreno et al. demonstrated somatic mutations in PRDM1(BLIMP1) in 50% of cases[21].
The largest series of transplant-associated PBL analyzed by next-generation sequencing detected genetic aberrations of the RAS/MAPK, TP53, and NOTCH signaling pathways[22].
Epigenomic Alterations
Hypermethylation of p16 has been reported in a case of PBL[12].
Genes and Main Pathways Involved
Put your text here and fill in the table (Instructions: Can include references in the table.)
The content below was from the old template. Please incorporate above.
MYC expression is suppressed by PRDM1 (BLIMP1) in terminally differentiated B cells; BLIMP1 encodes a transcriptional factor responsible for plasma cell differentiation[11].
The MYC activation present in PBL (by gene amplification or translocation) results in cellular proliferation and survival upon overcoming PRDM1 (BLIMP1) repression.
Genetic Diagnostic Testing Methods
Diagnosis is usually dependent on morphologic examination and immunohistochemistry demonstrating expression for plasmacytic antigens.
Conventional cytogenetics has utility in detecting MYC rearrangement and amplification. Most common translocation involves MYC -IGH.
Next-generation sequencing is helpful for identifying single nucleotide variants of PRDM1 and of genes in the of the RAS/MAPK, TP53, and NOTCH signaling pathways.
(use the "Cite" icon at the top of the page) (Instructions: Add each reference into the text above by clicking on where you want to insert the reference, selecting the “Cite” icon at the top of the page, and using the “Automatic” tab option to search such as by PMID to select the reference to insert. The reference list in this section will be automatically generated and sorted.If a PMID is not available, such as for a book, please use the “Cite” icon, select “Manual” and then “Basic Form”, and include the entire reference.)
↑ 2.02.1Campo, E.; et al. (2016). Plasmablastic lymphoma. in World Health Organization Classification of Tumours of Haematopoietic and Lymphoid Tissues. Revised 4th edition. Swerdlow, S.H.; Campo, E.; Harris, N.L.; Jaffe, E.S.; et al. Editors. IARC Press: Lyon, France. p 321-322.
↑ 8.08.1Campo, E. (2017). Plasmablastic neoplasms other than plasma cell myeloma. in Hematopathology. 2nd edition. Jaffe, E.S.; Arber, D.A.; Campo, E.; et al. Editors. Elsevier: Philadelphia. p 465-472.
*Primary authors will typically be those that initially create and complete the content of a page. If a subsequent user modifies the content and feels the effort put forth is of high enough significance to warrant listing in the authorship section, please contact the CCGA coordinators (contact information provided on the homepage). Additional global feedback or concerns are also welcome.
*Citation of this Page: “Plasmablastic lymphoma”. Compendium of Cancer Genome Aberrations (CCGA), Cancer Genomics Consortium (CGC), updated 11/3/2023, https://ccga.io/index.php/HAEM5:Plasmablastic_lymphoma.
.jpg)
.jpg)